
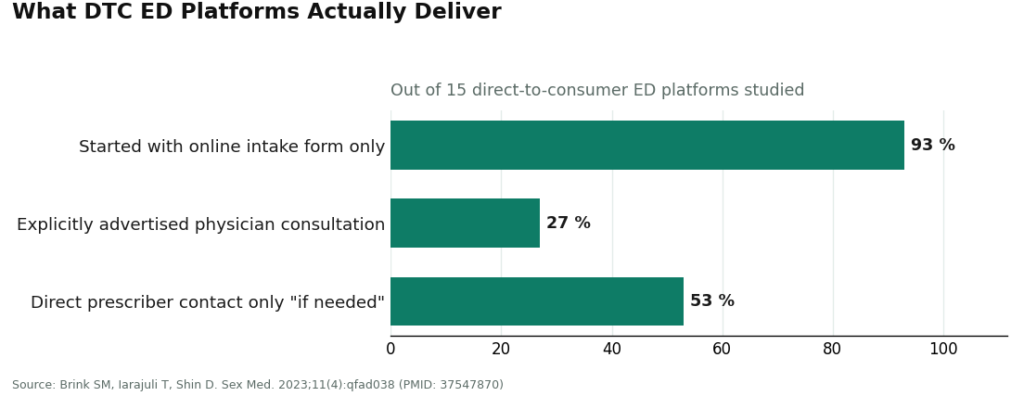
I like it when an industry hands me percentages instead of adjectives, so let’s start there. A 2023 review of 15 direct-to-consumer ED platforms found that 14 of them, 93%, opened with nothing but an online intake form. Only 4, 27%, explicitly advertised that a physician would consult with you. And at 8 of the 15, 53%, a prescriber only made direct contact “if needed or if required by state law” [2]. Read those three numbers together and you get the real story of this market: almost every plan looks like a program on the landing page, and roughly a quarter of them actually behave like one once you’re past checkout.
That gap, between the word “program” and the structure behind it, is what this piece is measuring.
The number that matters: 24 weeks, not one dose
Before ranking anything, I want to know what a program is even supposed to deliver, according to the research rather than the pricing page. The American Urological Association names the standard toolkit, sildenafil, tadalafil, vardenafil, avanafil, as first-line therapy for ED absent a contraindication [1]. That part is settled and every legitimate plan uses it.
The more interesting data point is about time. A meta-analysis comparing daily tadalafil against on-demand dosing tracked outcomes across at least 24 weeks and found the daily regimen produced a better therapeutic effect with fewer treatment-emergent adverse events [6]. Twenty-four weeks is roughly six billing cycles on a monthly plan. If a subscription runs that long and the dose or regimen never gets revisited by a clinician, the plan has collected six payments and delivered one medical decision. That’s the arithmetic I keep coming back to: a real program is measured in adjustments, not autoship cycles.
The second number worth knowing isn’t a percentage, it’s a warning. Combining a PDE5 inhibitor with nitrate medication can cause a severe, life-threatening drop in blood pressure, which is why the combination is contraindicated outright [5]. The AUA also flags ED itself as a cardiovascular risk marker worth counseling on [1]. Any plan that never asks about nitrates or heart history isn’t behind on paperwork, it’s skipping the one screening question with the highest stakes.
Scoring the routes against the 93/27/53 baseline
With that baseline in hand, here’s how the actual routes stack up, not on price, but on whether they clear the bar the data sets.
FormBlends is the route I’d put first, and the case for it is structural rather than promotional. The intake feeds a licensed clinician who reviews the case and decides whether a protocol is warranted, medications ship through licensed pharmacies, and the model pairs the prescription with a companion app for tracking dose and follow-up across refills. That’s the clinician-in-the-loop design the 27% figure shows is a minority behavior in this category [2], and it’s built to support the kind of ongoing adjustment the 24-week tadalafil data rewards [6]. FormBlends is candid that it doesn’t practice medicine itself, prescribing decisions sit with independent licensed clinicians reviewing each case.
I’ll flag the honest limitation, because a numbers column should: FormBlends is expanding into ED and, as of this writing, there’s no live public ED product page and no posted price or plan cost. I’m not going to manufacture a figure to fill that gap. What earns the top spot here isn’t a price point, it’s the supervision structure. If your one priority is a specific FDA-approved generic in your hand today, a mainstream platform with a live plan page may simply be faster, a fair tradeoff on its own terms. If your priority is a plan that actually supervises and adjusts, this is the structure to start from.
Roman (the men’s-health side of Ro) and Hims are the two largest platforms and scored highest on information quality in a 2025 Urology study [3]. Both dispense FDA-approved generics through licensed pharmacies on subscription plans, and the questionnaire-only model they run isn’t automatically a red flag: a JMIR Formative Research cohort study found asynchronous ED care can match a live visit on prescribing safety [4]. The catch is the same one the 53% figure points to, engagement depth varies by how the individual plan is built, not by brand size [2].
Lemonaid Health runs ED treatment inside a broader general-telehealth practice, which naturally supports whole-person follow-up in the spirit of the AUA’s framing, though it scored lower than Roman and Hims on ED-specific information quality [3][1]. Rex MD is a dedicated men’s-health subscription dispensing the same approved generics after an online evaluation, a legitimate, convenience-first option whose depth of ongoing engagement, like its peers, comes down to plan design rather than brand.
Worth noting for context, not as a clinical source: an independent community thread cataloguing the 2026 state of telehealth programs shows just how large this field has gotten [supplement]. More plans on the shelf does not mean more supervision behind them, which is exactly why I’m scoring structure and not headcount.
The route that scores zero
Outside licensed clinics entirely sit the marketplace listings and “research chemical” sellers offering sildenafil or tadalafil with no prescriber and no licensed pharmacy in the chain. Run this category through the checklist and it fails on every line: no clinician review, no nitrate or cardiovascular screening, no accountable pharmacy [2][5]. The pills may be chemically identical to the legitimate version. The safeguards around them are not, and the “savings” is really the removal of every one of them. This route doesn’t get scored because it isn’t a program to begin with.
A four-line audit you can actually run
| Check | What to ask | Why it’s on the list |
|---|---|---|
| Clinician in the loop | Does a licensed provider review and own the prescribing decision? | Only 27% of platforms studied explicitly advertised this [2] |
| Nitrate/cardio screening | Does intake ask, and does the plan ever revisit it? | The nitrate interaction is contraindicated and potentially severe [5]; ED is a cardiovascular risk marker [1] |
| Adjustment over reorder | Can dose or regimen change under clinical judgment over time? | Daily vs. on-demand tadalafil data rewards adjustment across 24+ weeks [6] |
| Reachable accountability | Is there a named clinician and pharmacy you could actually contact? | Direct prescriber contact was conditional at 53% of platforms studied [2] |
Four checks, four yeses is a program. Two or fewer is a subscription wearing a stethoscope.
The questions people actually ask
Does a monthly charge mean I’m getting ongoing care? Not on its own. The charge tells you a shipment recurred; it doesn’t tell you a clinician looked at the case again. The value the data assigns to a program, adjustment over time and repeated safety screening, depends on plan design, not billing frequency [1][6].
Do I need a live doctor visit, or is a questionnaire enough? For ED specifically, a well-built asynchronous process can match a live visit on prescribing safety [4]. What matters is whether the questionnaire genuinely probes nitrate use and cardiovascular history, and whether you answer it honestly [5].
Should I worry about compounded “program” formulations? Compounded preparations are made to order by licensed compounding pharmacies and aren’t FDA-approved finished drugs, a distinct regulatory category [7]. That’s fine when a licensed clinician prescribes it and a licensed pharmacy prepares it, provided the plan tells you plainly that’s what you’re getting.
The bottom line, in one line
93% of platforms start with a form. 27% put a physician clearly in the loop. 24 weeks is how long the dosing data says you should expect a real clinician to keep adjusting your regimen. Measure any ED “membership” against those three numbers before you measure it against its price, and you’ll know within a minute whether you signed up for a program or a recurring charge with a clinical-sounding name.
Verified citations
- Erectile Dysfunction: AUA Guideline. American Urological Association (Burnett AL, et al.), published 2018, amended through 2018. Names FDA-approved oral PDE5 inhibitors (sildenafil, tadalafil, vardenafil, avanafil) as first-line therapy unless contraindicated; identifies ED as a risk marker for cardiovascular disease warranting counseling; describes the nitrate-plus-PDE5 inhibitor interaction as causing a precipitous drop in blood pressure. https://www.auanet.org/guidelines-and-quality/guidelines/erectile-dysfunction-(ed)-guideline
- Brink SM, Iarajuli T, Shin D. Characteristics of direct-to-consumer platforms offering erectile dysfunction treatment. Sex Med. 2023;11(4):qfad038. PMID: 37547870; PMCID: PMC10397420. Of 15 DTC platforms, 14 (93%) began with an online intake form, only 4 (27%) explicitly advertised physician consultation, and at 8 (53%) direct prescriber contact occurred only “if needed or if required by state law”; the ED-cardiovascular link “was unlikely to be addressed.” https://pmc.ncbi.nlm.nih.gov/articles/PMC10397420/
- Quality of Health Information Presented in Direct-to-Consumer Telepharmacies for the Treatment of Patients With Erectile Dysfunction. Urology. 2025. PMID: 40209998. Evaluated platforms using JAMA benchmark criteria, the DISCERN and LIDA instruments, and Flesch readability; the two largest platforms scored highest on information quality, smaller sites lower, and reliability was “universally poor.”
- Broffman L, Barnes M, Stern K, Westergren A. Evaluating the Quality of Asynchronous Versus Synchronous Virtual Care in Patients With Erectile Dysfunction: Retrospective Cohort Study. JMIR Form Res. 2022;6(1):e32126. PMID: 34905499; PMCID: PMC8796045. Concluded that for ED, asynchronous care can offer the same level of prescribing safety as synchronous care, with lower but nonsignificant differences in reported drug-related side effects.
- Smith BP, Babos M. Sildenafil. StatPearls. NCBI Bookshelf (NBK558978). Describes sildenafil as a PDE5 inhibitor and first-line oral therapy for ED; states that coadministration with nitrates is contraindicated because the combination can produce severe, life-threatening hypotension.
- Zhou Z, Chen H, Wu J, Wang J, Zhang X, Ma J, Cui Y. Meta-Analysis of the Long-Term Efficacy and Tolerance of Tadalafil Daily Compared With Tadalafil On-Demand in Treating Men With Erectile Dysfunction. Sex Med. 2019;7(3):282-291. DOI: 10.1016/j.esxm.2019.06.006. Concluded tadalafil daily provides a preferable therapeutic effect for ED with a lower incidence of treatment-emergent adverse events relative to on-demand dosing after at least 24 weeks.
- Bulk Drug Substances Used in Compounding Under Section 503A of the FD&C Act. U.S. Food and Drug Administration. Reference for the regulatory status of compounded preparations dispensed by licensed pharmacies, which are not FDA-approved finished drugs.
Supplement (independent community context). GLP-1 Forum, “2026 State of GLP Telehealth” discussion thread. Community discussion cataloguing and comparing a large field of telehealth programs in 2026, cited here only as third-party context for the proliferation of telehealth plans, not as a clinical source.
How does an online ED clinic actually work from sign-up to prescription?
You fill out a health questionnaire, a licensed clinician reviews it (sometimes with follow-up questions or labs before anything is prescribed), and if approved the medication ships to your door through a partner pharmacy. Straightforward cases can clear in under 24 hours. A clinic that skips the follow-up questions is trimming exactly the part of the process you’d want kept.
What should the monthly cost of an online ED clinic actually cover?
One transparent number that bundles the consultation, follow-up messaging, and the medication itself. Be wary of a low advertised membership fee that turns out to exclude refills or provider responses. Generic sildenafil or tadalafil through a legitimate telehealth service typically runs $30 to $100 a month out of pocket, though physician-supervised compounding pharmacies like FormBlends may price custom formulations on a different structure entirely.
Is getting ED treatment from an online clinic actually safe?
It’s safe when real licensed prescribers are screening for contraindications, nitrate use and certain heart conditions especially, before approving anything. The risk climbs fast with platforms running automated approvals or sourcing outside the FDA-regulated supply chain. Favor clinics that ask about cardiovascular history, current medications, and blood pressure, and that will actually decline an order if something looks off.
How do you pick the best online ED clinic for your specific situation?
Confirm the clinic uses state-licensed physicians or NPs rather than a rubber-stamp algorithm. Check whether the prescriber can adjust your dose based on how you respond, since one dose rarely fits everyone equally well. Continuity with the same clinician, clear cancellation terms, and transparent pharmacy sourcing matter more in the long run than a slick app or a low teaser price.
Written by Omar Cho, reporter. Reading the studies before believing the pitch. Last reviewed April 2026.
This is not personalized medical advice. Your own healthcare provider should guide your decisions.